Refractive lens exchange (RLE)
Someone who has a “normal sighted eye” is able to see well at all distances both for near visual tasks such as reading a book and in the far distance such as looking at the horizon.
There are two lenses at the front of the eye that focus light onto the retina or photographic film at the back of the eye.
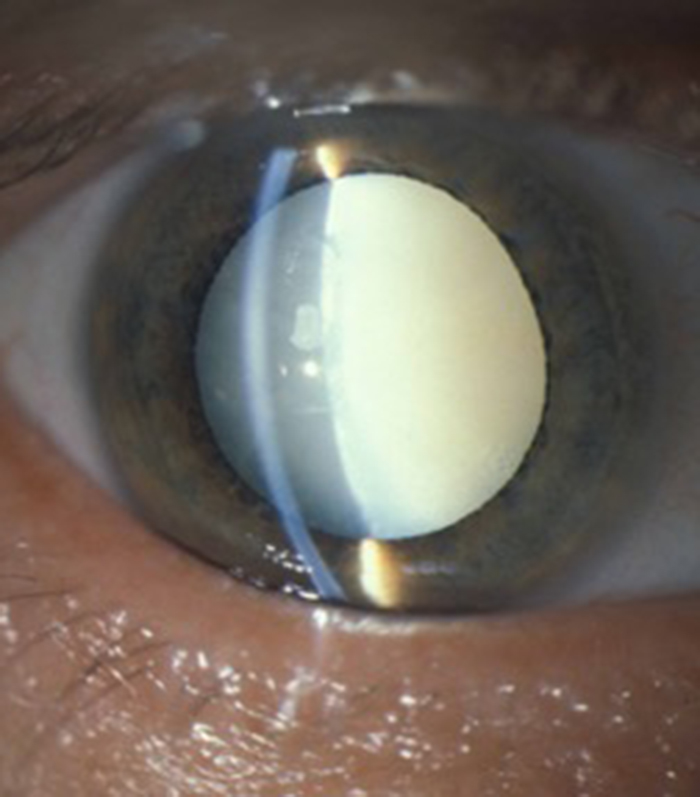
The main focus is the cornea or clear window at the front of the eye which does 2/3rd of the focus. The cornea is a fixed focus mechanism and cannot change its focus. The second lens is called the crystalline lens and is inside the eye. This is the lens that goes cloudy when you have a cataract. This is the fine focus and contributes the remaining 1/3rd of the focus of the eye. The crystalline lens however can increase its focus by changing its shape (a process called accommodation) and this allows you to focus for near (when increased focusing power is needed) as well as distance (when the crystalline lens is in its relaxed, at rest position).
This accommodative or focusing power for near reaches its peak at the age of about 18 and then starts to deteriorate. Fortunately we have plenty of accommodation “in reserve” but by the age of 45 to 50 this reserve runs out, our arms are not long enough, and we have to reach for reading glasses.
We are not all the same shape and size and our eyes are also variable in their shape and size. This can result in a variety of problems with focus and the three main problems are shortsightedness (myopia), longsightedness (hypermetropia) and astigmatism. I will now describe each in term.
What is short-sight, long-sight and astigmatism?
Most patients who are short sighted (myopic) have larger eyes. This means that when looking into the distance (such as the horizon) the light unfortunately focuses in the middle of the eye and not on the retina. This is why the distance is blurred. It often is spotted when children go to school and struggle to see the white board (or blackboard in the good old days!) at the front of the class. If however you are short sighted you are in focus (the light rays fall on the retina) when looking at near objects. The more short sighted you are, the closer you have to hold the object you are looking at in order for it to be in focus.
Most patients who are long sighted “hypermetropic” have small eyes. This means that when looking into the distance (such as the horizon) the light unfortunately wishes to focus at a point behind the eye and not on the retina. In younger patients who have large reserves of accommodation the crystalline lens inside the eye can accommodate (normally only needed when looking at near objects) to get the distance into focus and accommodate even more to get near objects in focus. This can result in eye strain and patients who are long sighted will need glasses for distance and near when their power of accommodation can no longer keep things in focus.
If you have astigmatism the problem does not relate to the eyes being too big or too small but is associated with the shape of the cornea. As mentioned before the corneal does most of the focus of the eye (2./3rd of the focus or the coarse correction) but it is a fixed focus system with the crystalline lens inside the eye being able to change its focus (accommodate) to enable focusing at different distances.
The significant focusing power of the cornea is the reason why contact lenses placed on the surface of the cornea can have such an effect on correcting focusing problems in the eye.
For the cornea to work as an optical lens with perfect focus it needs to be equally curved in all directions (as if it is part of a sphere or football). If astigmatism is present the cornea is more curved in one direction than the other (as if it is rugby ball shaped). If significant astigmatism is present it results in blurring of vision at all distances.
Short-sight, long-sight and astigmatism can all be corrected optically with either glasses or contact lenses. If you are seeing well and are comfortable with your glasses or contact lenses you should read no further. Refractive surgery has its risks and if you are not troubled I would not advise surgical intervention.
Removal of the crystalline lens inside the eye (refractive lens exchange or RLE) and replacing it with an intra-ocular lens can treat short-sight, long-sight and astigmatism. It will also however completely remove any remaining accommodation (the ability to change focus at different distances) so I feel it is only suitable for patients who have reached an age where accommodation has significantly declined or been lost completely (usually over age 50).
What are the options?
If you are short sighted RLE surgery can make you normal sighted. This will make you see well in the distance but you will need glasses for reading. This requires an intra-ocular lens called a monofocal lens which gives excellent optics at a set distance (the far distance).
If you are long sighted RLE surgery can make you normal sighted. This will make you see well in the distance but you will still need (weaker) glasses for reading. This requires an intra-ocular lens called a monofocal lens which gives excellent optics at a set distance (the far distance).
If you have astigmatism RLE can make you normal sighted. This will make you see well in the distance but you will still need glasses for reading. This requires an intra-ocular lens called a toric lens which counterbalances the uneven cornea and which gives excellent optics at a set distance (the far distance).
What if I want to do away with reading glasses too?
This is where multifocal or extended depth of focus lenses may be used. It is important to realise at this juncture that up to now the lenses used to correct short sight, long sight and astigmatism (monofocal and toric lenses) have very high quality optics and produced very good vision as they take all the light that is entering the eye and concentrate it at a single focus on the retina. The current lenses that are available and reduce requirement for reading glasses all have the same property of “sharing” the light that enters the eye with a certain amount being used for near, intermediate and far distance focus. This sharing of light slightly degrades the quality of each image falling on the retina. In good light this effect is hardly noticeable but in reduced light such as twilight it may have a greater effect. Most multifocal or extended depth of focus lenses work very well but it mainly reduces dependance on glasses for reading rather than being completely spectacle independent. Patients may still need to wear weak reading glasses if they are looking at small print which is not black on white in a dimly lit restaurant
These lenses are also slightly more prone to producing glare and halo effects around point light sources such as oncoming car headlights.
They work best when the eyes are otherwise healthy, any astigmatism has been corrected by a toric component to the lens and the intra-ocular lens is implanted in both eyes. They should also be used with caution if you have had previous refractive laser eye surgery (due to difficulty in getting very accurate measurements of the corneal shape after refractive surgery). Patients who are previously myopic (short-sighted) and are used to having very good near vision without glasses may also be a little disappointed with the quality of near vision that these lenses produce although are usually happy at the good distance vision without glasses.
Patient selection is therefore paramount when using these multifocal and extended depth of focus lenses and requires an in-depth discussion of risks and benefits for you as an individual with your particular requirements.